06 · Peer notes
If you've just been diagnosed, read this
What follows is peer advice from someone who lived it. It is not medical
advice. If anything below contradicts your doctor, follow your doctor. The whole
point of this page is that you have to do the reading yourself and decide with a
qualified clinician.
Don't let it get into your head
The mental damage you can do to yourself is bigger than the disease. I went
through it. Anxiety, obsession, scanning yourself a hundred times a day for
changes, that loop will hurt you more than the plaque ever will. Step out of
it. Live a normal life. Treat the protocol as the work; treat your day as your
life. Don't measure the curvature every morning. Don't catastrophise. The disease
rewards calm patience much better than it rewards panic.
And the questions are going to come. Will I ever find a partner now? Will
I ever have a family? Will my current partner stay? Will I have sex again, or
was that it? Will I be the same person in bed afterwards? Do I have to be
operated, and what will be left of me if I am? They come at three in the
morning. They come in the shower. They come every time you see a couple in
the street. Recognise what they actually are: the spiral the diagnosis
produces, not the answers it has. The honest answers, on the data this page
is built on, are: yes — yes — probably yes — almost certainly yes —
very likely yes — and most likely no. Most men on conservative
therapy in the active phase do not end up at surgery. Most partners do not
leave. Most sex lives recover. Some recover entirely. The catastrophic version
of this story is overwhelmingly not the version that plays out, and treating
the catastrophic version as the working assumption is itself one of the
biggest accelerators of harm. Notice the spiral, name it, and put the question
down. The work you can actually do today is take the protocol, sleep, eat,
move, talk to someone you trust. Tomorrow's answers will arrive on their own
schedule and will mostly be kinder than the version your three-in-the-morning
brain is offering you.
You can, and should, keep having sex
If the curve isn't severe enough to make penetration impossible, and pain isn't
blocking it, keep your sex life normal. Date normally. Communicate with partners.
Have intercourse if you both want to. The disease can heal while you live.
It does not require monastic abstinence. Withdrawal from intimacy is one of the
biggest hidden costs of this diagnosis, and most of it is self-inflicted.
If penetration isn't possible right now, read this
The previous note assumes the curve still allows penetrative sex. If it
doesn't, pain blocks it, the angle blocks it, rigidity blocks it, the
following anatomy takes most of the weight off you. Internalise it
properly and the temporary loss of penetration stops feeling like a loss
of your sex life.
Most women do not orgasm from vaginal penetration alone.
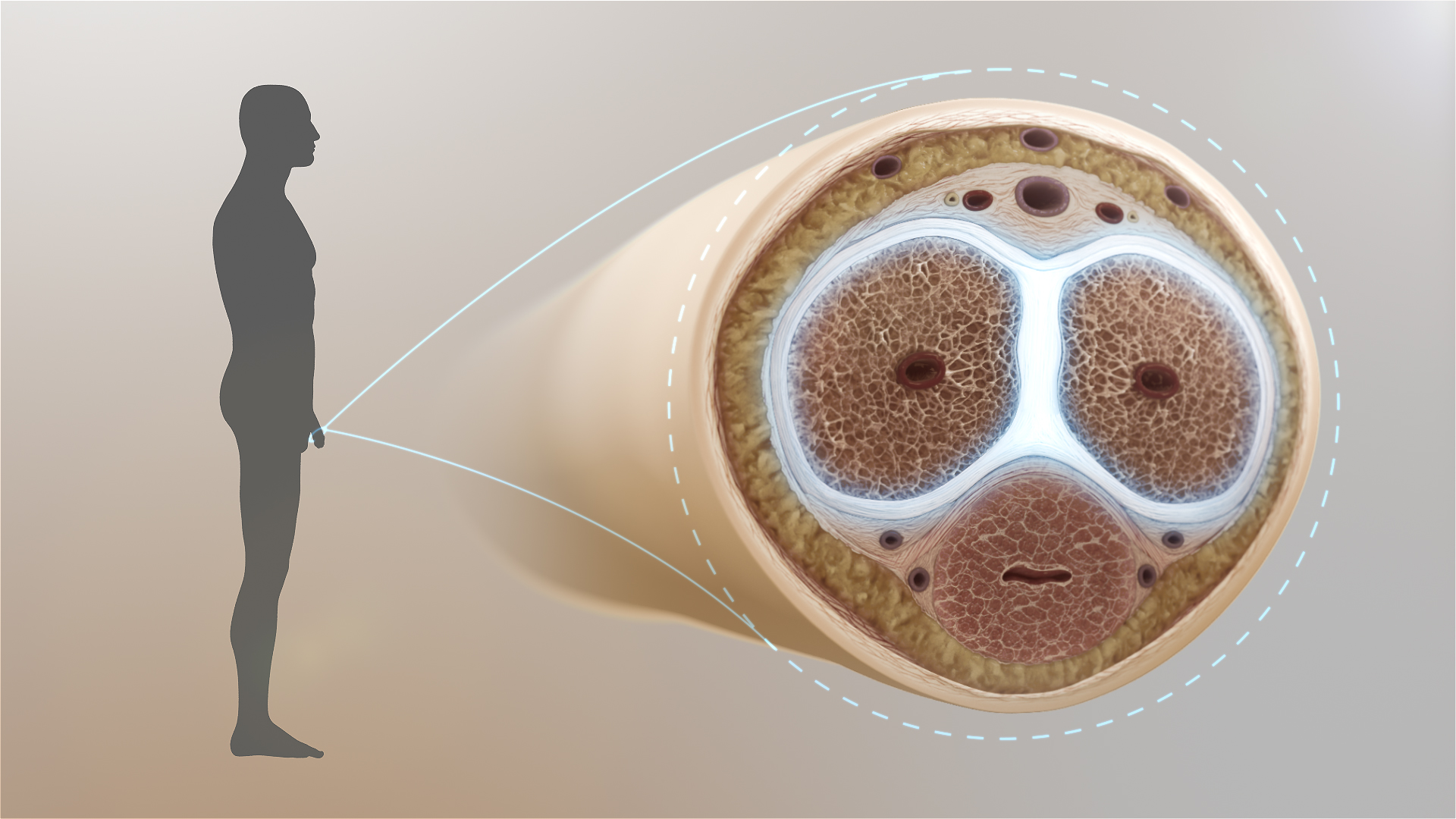
The clitoris
is far larger than the visible glans, it has internal "legs" called the
crura that wrap around the vaginal canal, plus the vestibular
bulbs. When a woman feels a "vaginal" or "G-spot" orgasm, the underlying
physiology is almost always the internal clitoral structure being
stimulated through the vaginal wall. The visible glans clitoris remains by
far the most reliable, most innervated trigger. Population studies
consistently put the proportion of women who reliably orgasm from
intercourse alone at roughly 18–25%.
Penetrative sex, in other words, is mostly fun you want to have.
For her it is frequently optional, pleasant if it is good, but not the
physiological route to her orgasm. The cultural script that says "real sex
equals penetration, everything else is foreplay" is wrong about the
biology. Direct clitoral stimulation, fingers, mouth, toy, hand, works
for the great majority of women, with or without your penis being part of
the picture. While your tunica is healing, lean into that. Communicate,
ask what she actually likes, focus on her, and the curvature stops being a
sex-life problem and goes back to being only a healing problem.
Your side of the equation is just as flexible. You do not need to
be the one penetrating to have an orgasm. Glans stimulation by
her hand, oral sex / blowjobs, mutual masturbation, frottage, toys used on
you, every one of these is a perfectly normal route to orgasm and
ejaculation, and most of them put zero buckling stress on the tunica
while it heals. Penetration is one option among several for both partners
, not a prerequisite for either of you to come, to have sex, or to feel
intimate and satisfied together. The same is true for gay couples,
people in transition, and other cases: when receptive or insertive
intercourse is temporarily off the table, oral, manual and toy-based
routes get you both to the same destination without the mechanical risk
to a healing plaque.
And, peer to peer, don't be hard on yourself. Be hard for your
partner.
On coffee, timing, and consistency
Coffee is fine. One or two cups a day does not conflict with the
protocol; you do not need to give it up. What matters far more than
coffee is taking the oral compounds twice daily on an empty
stomach, every day, without skipping. Peyflog in particular is
prescribed two tablets twice daily on an empty stomach (four tablets
total per day), and the rest of the oral stack follows the same
morning / evening rhythm. The antioxidant exposure has to be continuous
for the cascade on this page to stay suppressed; intermittent dosing is
the single most common reason a protocol stalls. Set two fixed times,
first thing on waking and last thing before bed are the easiest, leave
a 30-minute to 1-hour gap before food, and treat it like brushing your
teeth.
On pain, and the NSAID + Tadalafil caution
Topical diclofenac
on the plaque is the first move for local pain. If you are tempted to take an
oral NSAID on top of it, talk to your doctor first. Daily
Tadalafil 5 mg already has a baseline cardiovascular load (it lowers blood
pressure); oral NSAIDs add their own (BP, fluid retention, thrombotic risk).
Combining the two without supervision is a needless double burden. This is
exactly the kind of decision that needs a clinician in the loop. None of this
page is a substitute for that conversation.
Healing chances are better when…
…you are younger, leaner, non-diabetic, and don't carry other diseases,
metabolic, vascular, autoimmune, that maintain a pro-fibrotic /
pro-oxidative baseline. Those comorbidities act as constant upstream
triggers: they keep refilling the ROS / TGF-β1 reservoir while you are trying to
drain it. Treat them in parallel. Get the basics measured,
prolactin,
25-hydroxy vitamin D,
fasting glucose / HbA1c, lipid panel, free testosterone. Address what comes
back abnormal. The protocol is much more powerful when the baseline isn't
actively working against it.
Lifestyle adjustments I would recommend
None of this is groundbreaking, none of it is contested in the literature,
and most of it costs nothing. It moves the needle anyway, because every
item below either lowers the oxidative / inflammatory floor or removes a
constant trickle into the cascade described on this page.
-
Move, but moderately. Steady-state cardio: running,
jogging, brisk walking, swimming, cycling at conversational pace.
Three to five sessions a week is plenty. Avoid extreme exertion
during the active phase, competitive sports, heavy contact sport,
maximal-load lifting. Extreme exertion spikes systemic ROS and adds
mechanical strain; you do not want either right now. Moderate movement
improves endothelial function, lowers fasting glucose, lowers
background inflammation, and improves nocturnal erections.
-
Drink water. Properly hydrated tissue handles
oxidative load better and supports the renal clearance of
metabolites the antioxidant stack is mobilising. Aim for the colour
of pale straw in your urine; that is roughly the right amount for
you.
-
Cut alcohol back. Alcohol is metabolised through
aldehyde intermediates that consume the same antioxidant pool you are
trying to refill, and it suppresses nocturnal erections for the
following 24–48 hours. Occasional and modest is fine; daily or
heavy is not.
-
Stop smoking. Tobacco is a continuous oxidative and
vasoconstrictive insult to exactly the cavernous tissue you need
functioning. If you smoke, this is the single highest-leverage
lifestyle change you can make alongside the protocol.
-
Remove or reframe your psychological stressors.
Chronic stress keeps cortisol, sympathetic tone and inflammatory
cytokines elevated, all of which feed the same loop. Identify what is
actually stressing you. Remove what can be removed. Reframe what
cannot, therapy, journalling, an honest conversation with the
partner / family member / boss involved. Do the work. It is
medically relevant in this disease, not optional.
-
Therapy if you need it. A diagnosis like this
dropped on you is genuinely a lot to carry. A few
months of cognitive behavioural or psychodynamic therapy is among
the most cost-effective interventions you can buy yourself during
treatment. Even informal alternatives count: long walks alone with
your thoughts, regular reflection, a journal, a trusted friend who
will actually listen. Anything that lets the mental load discharge
rather than accumulate.
-
Listen to your body. If something, a food, a
position, a routine, consistently feels good and coherent, do what
feels right for your body, as long as it doesn't conflict with the
therapeutic protocol. If something feels off, take it seriously and
investigate before dismissing it. The signal-to-noise ratio of your
own interoception during this period is unusually high; pay
attention to it.
Postscript, if the protocol is working you may feel mildly
unwell on some days during the first weeks or months: low energy,
dull headaches, vague fatigue, the impression of a low-grade flu without
any actual infection and with bloods that come back clean. That is
commonly reported on starting a dense antioxidant / anti-inflammatory
stack, interpret it as the system rebalancing under genuine
intervention, not as the protocol "not agreeing with you." It passes.
Get yourself tested. Properly., and use condoms
This one I am going to be blunt about, because most men reading this will
not have done it and the cost of skipping it can be the disease itself.
Get tested for bacterial STIs, urethral swab, first-void urine PCR,
seminal-fluid culture, and a glans / coronal-sulcus swab if anything looks
irritated. Not just the standard quick STI panel: the
sub-clinical chronic infections, Chlamydia trachomatis,
Mycoplasma genitalium, Ureaplasma urealyticum / parvum,
atypical Neisseria, occasional anaerobes from the partner's
flora, frequently smoulder for years in men with no urethral discharge,
no burning, no obvious symptoms. They are routinely tested for in women
during gynaecological care; they are routinely missed in men
because no one ever swabs us. A chronically infected urethra or
seminal-fluid compartment is exactly the kind of low-grade systemic
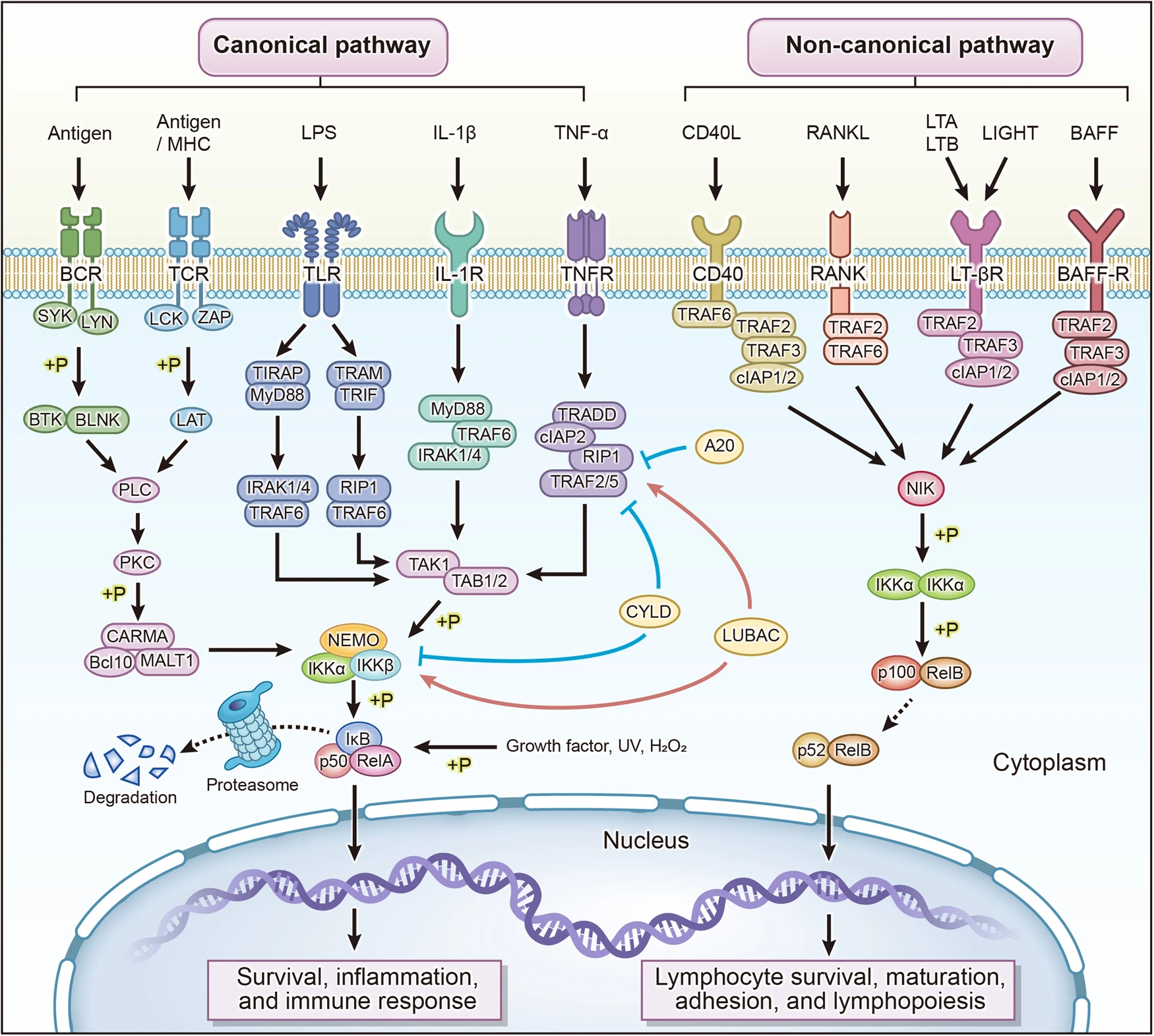
inflammatory stimulus that keeps the NF-κB / TGF-β1 floor elevated and
prevents conservative therapy from getting traction. Test, treat with the
right antibiotic if positive, and re-test to confirm clearance. Do this
once at the start of the protocol and again if anything stalls.
And, basic knowledge most adult men still ignore, use
condoms. With every new partner, until both of you have a clean
recent panel and have had a real conversation about it. The guys who
skip this are the same guys who end up with the chronic
urethritis they don't know they have. None of this is moralising; it is
simply mechanism. Bacterial inflammation drives oxidative stress,
oxidative stress drives the cascade on this page, and the cascade gives
you a curve. Take it seriously from here on, buddy.
On erections during the active phase
Tadalafil 5 mg
once daily is a long-term-safe regimen in patients without contraindications,
nitrate use, severe hypotension, recent cardiovascular events, severe hepatic /
renal impairment. Read the contraindications honestly, take the prescription if
you fit. A reasonable erectile life during the active phase actively helps the
protocol: nocturnal erections oxygenate cavernous tissue and oppose the fibrotic
signal. Avoidance and disuse make things worse, not better.
If you can travel to Rome, go
Paulis is, in my opinion, the first-line treatment for Peyronie's disease
worldwide, and that is not casual praise. He is the
inventor of the multimodal antioxidant approach to PD: he
published the rationale in the early 2010s, refined the protocol across a
decade of clinical case series, and has been the
perfector of it ever since, iterating dosing, sequencing
and individual adjustments through hundreds of treated patients. He is
the only andrologist I am aware of who has published case series of
complete plaque regression on conservative therapy
(J Med Case Rep 2022;
Am J Case Rep 2022).
Search PubMed yourself, that's not a soft claim, it is checkable. Until
other groups replicate his outcomes in print, the rest of the andrology
world's surgical-first orthodoxy should be treated with healthy
skepticism for anyone still in the active phase.
The reason to actually go, not just buy the compounds online,
is that your individual case can only be reliably treated by him,
not by his stack alone. Two patients with the same nominal
diagnosis differ in plaque morphology, phase, hormonal milieu,
comorbidity profile, response trajectory and the upstream drivers
keeping the cascade fed. Paulis adjusts the protocol, dose, timing,
sequence, additions, substitutions, to that individual signature. That
is what makes the difference between a generic regimen and the
targeted multimodal therapy his published outcomes are based on. For
most patients the stack works as documented and is effectively
plug-and-play, but for a meaningful minority, the cases with awkward
comorbidities, atypical phase presentation, or upstream drivers that
keep refilling the cascade, it is not, and individualisation is exactly
what separates a good outcome from a stalled one.
Diagnosis is the other half of it. The protocol is only as good as the
imaging it is built on, and proper imaging is itself a specialty,
B-mode ultrasound + colour Doppler + real-time elastography of the
flaccid penis, performed by an experienced operator with a
sufficiently advanced machine, exactly as Paulis' 2022 case series
explicitly demands. The ultrasound at his clinic is performed by
Giovanni De Giorgio, an expert ultrasound and
elastography operator and Paulis' co-author on the 2012, 2022 and 2025
papers; Paulis then does consultation and treatment. Two doctors, both
sub-specialised, both publishing in this exact field. That is what a
proper diagnosis of Peyronie's looks like, not a single Doppler scan
in a urology clinic that sees the disease three times a year.
The visit itself is structured the way every serious specialist clinic
works: ultrasound by one doctor, consultation and treatment by another,
with first appointments longer than follow-ups. Fees are not posted
publicly and you should ask the clinic directly. Done smartly from most
EU countries, however, the entire trip, flight, one night in a
modest hotel, train or metro to the clinic and the consultation itself,
can come in under €500 total. That is in another universe of
price-point from a single Xiaflex cycle, an ESWT course, or penile
surgery, let alone the lifetime cost of a prosthesis.
And, quite apart from the medicine, Rome is an extraordinary place to
be when you are trying to put yourself back together. Walk a city
whose stones have been laid down across two and a half thousand years.
Sit in piazzas that were built before your country existed, eat
properly, the Italian Mediterranean diet is, incidentally, exactly
the anti-inflammatory eating pattern this protocol thrives on, drink
an espresso looking at the Pantheon, take a slow evening along the
Tiber, climb up to the Aventine for sunset. Every day in Rome, even
between appointments, lowers your cortisol in a way that no amount of
sitting at home and worrying about your curvature ever will. Take the
trip as a life experience, not just a medical errand. You will come
home with the beginning of healing in your tunica and a real
memory of one of the most beautiful cities on earth, that is a much
better souvenir than the average diagnosis lets you bring home.
And the obvious joke, because it is too good not to write it down:
every andrologist on earth will tell you that all roads lead to
surgery. They do not. One of them leads to Rome.
If you cannot get the actual manufacturer products
Peyflog, Alpavita EC, Alpavir Uno and Sclero-Hyal can be ordered
online from anywhere; that part is not a travel question. The real
constraint is if those specific manufacturer products are genuinely
unavailable to you, customs blocks, regulatory limits in your country,
the manufacturer pausing distribution, whatever the reason. In that case
the protocol can still work, but only if you reproduce it precisely from
individual components. Same actives. Same titrations and formulations as
the manufacturer products listed above. Same dosing schedule.
All of them present together. Remove one, say, skip the
topical because you don't like creams, or drop CoQ10 because it's the
most expensive line, and you are dismantling a network effect.
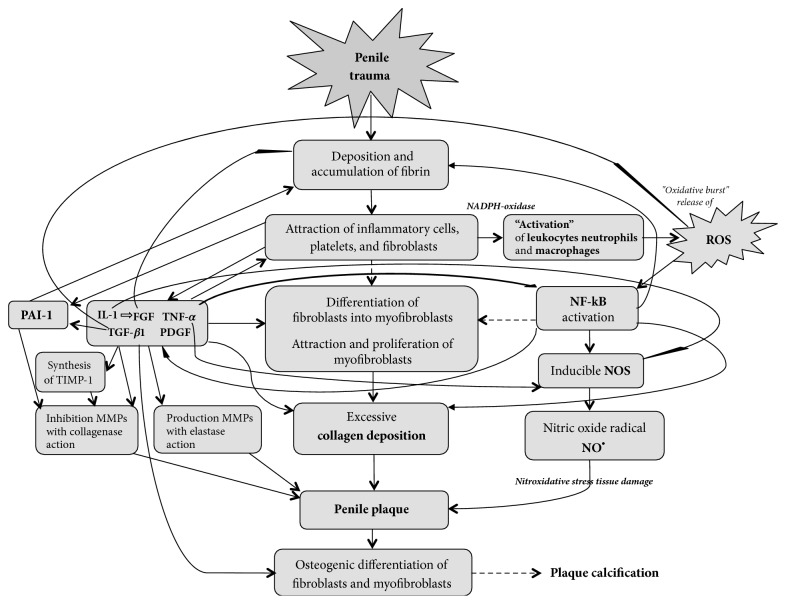
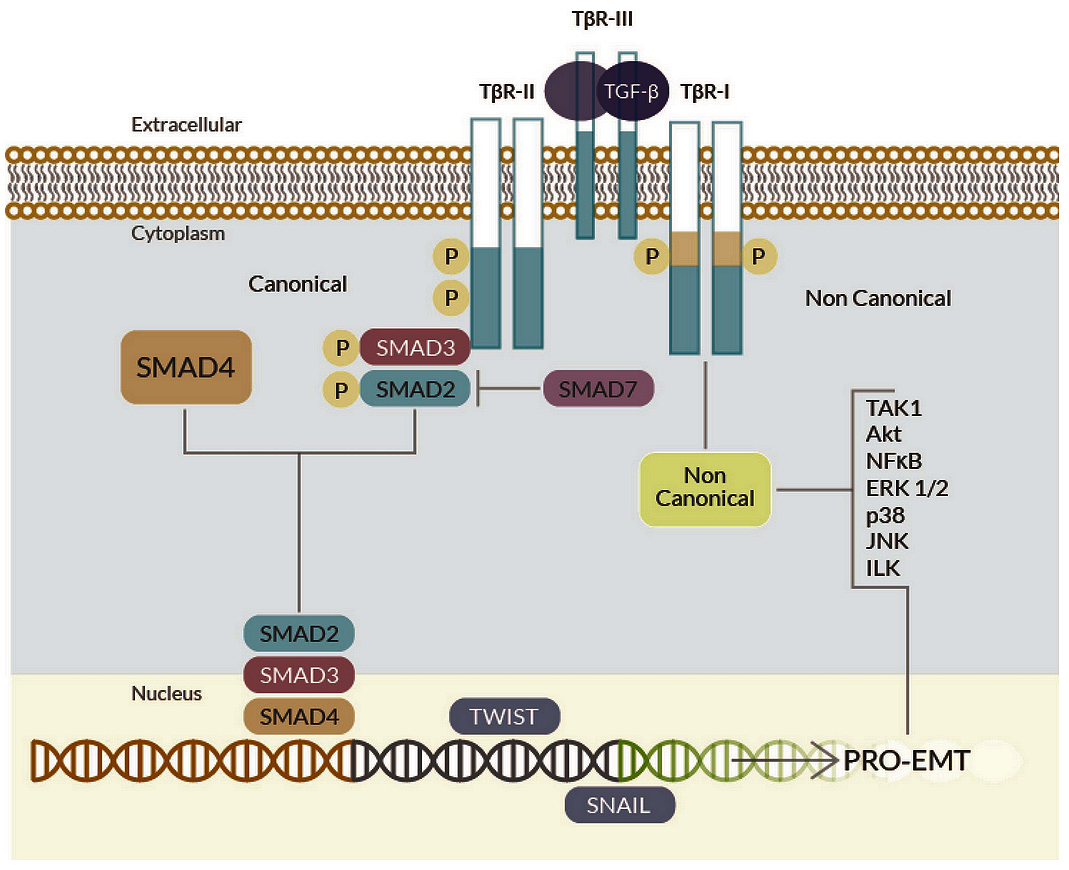
Each compound covers a node the others don't. As the cellular section
of this page shows, the rationale is genuinely synergistic: ROS is
damped here, NF-κB suppressed there, TGF-β1 modulated laterally,
NO/cGMP sustained from the other side. Take everything, or expect
proportionally diminished results.
A word on Paulis, and on Pisa
Most of the andrology world treats Peyronie's as a disease that can only
be debrided, sliced, or implant-replaced. Paulis treats it as what it
actually is, a chronic inflammatory and fibrotic disorder that obeys the
same rules as any other fibrosis, and that responds, like any other
fibrosis caught early, to sustained redox + anti-inflammatory pressure
plus time. That insight is, in my private opinion, a piece of frontier
medicine. He invented the multimodal antioxidant framework for
Peyronie's, has spent more than a decade perfecting it across
published case series, and remains one of very few clinicians anywhere
translating it into a daily protocol that ordinary patients can actually
run.
His credentials are worth understanding. Medicine and Surgery,
La Sapienza Rome. Specialty in Urology (Rome, 1985). Specialty
in Endocrinology, field of Andrology, at the
University of Pisa (2002), plus a separate University
Masterclass in Andrological Ultrasonography also at
Pisa. The University of Pisa is one of Italy's oldest universities
(founded 1343) and operates the country's flagship Endocrinology-Andrology
specialty programme, the most rigorous integrated training in
reproductive endocrinology, sexual medicine and dedicated andrological
imaging available in Italy. That is why a Paulis consult is structurally
different from any standard urology visit: hormonal axis, tunica
biochemistry and high-resolution ultrasound of the plaque are thought
about by the same person, in the same room, on the same day. Few
clinicians in the world combine all three.
Read
his PubMed publication record.
Form your own view.
Last thing
If you have just been diagnosed and you are scared: take a breath. The
literature is on your side, the protocol is on your side, your own biology is
on your side if you treat it well. Be good to yourself. Work toward happiness
independently of how the curvature looks tomorrow. That is the only thing
actually in your hands, trying everything you can, and being happy regardless
of the outcome. Most of the men reading this will get their lives back. Some
will not. Either way: live well.
.png)
.png)